Committee on Economic Security (CES)
"Social Security In America"
Part III
SECURITY FOR CHILDREN
Chapter XV
MATERNAL AND CHILD-HEALTH SERVICES
THAT any program for the promotion of the health of mothers and children as part of a total program for greater social and economic security for children should be closely coordinated with a general program for public health, such as has been proposed by the Public-Health Committee, advisory to the Committee on Economic Security, is obvious. The great need for expansion of the program is evident. At the beginning of 1935 there were 8,000,000 children under 16 years of age in families an the relief rolls and probably as many more in families on the border line of relief. There is evidence that many children in these groups were not getting the medical care they needed, either in sickness or for the correction of remediable defects which handicap growth, and that many were undernourished. Among adolescents were found evidences of increasing mental instability and inability to meet the problems that arise from unemployment and depleted family resources.
To some extent the need for expansion of the program for promoting the health of mothers and children can be measured by mortality rates, especially those of certain groups of the population; it may be estimated from reports of morbidity and lack of medical care among mothers and children; or it may be judged by the social disaster that takes place yearly in the thousands of homes where the death of the mother in childbirth leaves one or more children to be cared for by others. Though favorable social and economic conditions are undoubtedly important underlying factors in reducing infant mortality and in maintaining the health and permitting normal growth of children, the part that can be played by educational and health services in further reducing infant-mortality rates and improving child health under favorable economic and social conditions, or in mitigating the effects of bad conditions, has been demonstrated sufficiently to warrant the conclusion that increased and more widespread effort would be justified. If deaths of infants and mothers are to be prevented and the level of child health is to be raised, not only must there be improvement in those economic and social conditions that make for a better standard of living, but provision must be made for better maternal care, for increasing our knowledge of causes of deaths.
260
among newborn infants, for providing more adequate facilities for the care of newborn infants (especially of those prematurely born), for extension of the well-known educational and service programs for infants and young children, and for further control of communicable diseases and community milk and water supplies and development of other general public-health measures.
Just as there is a lag in the appearance of the effects of widespread economic disaster on general mortality rates, so also may the effects of general educational and service measures be gradual in making their appearance. It is important, therefore, that the program for promotion of the health of mothers and children be a continuous one, planned especially to reach those population groups which are most in need. When economic conditions are unfavorable, as they are today, for large groups of the population, the need for an expanded program of education and service to protect the lives and health of mothers and children is even greater.
Available data with regard to maternal and infant deaths and mortality rates, the health and nutritional condition of children, and resources for maternal and child-health work in the States are given in this chapter. These indicate the need for special effort in rural areas and among certain groups of the population.
MATERNAL AND INFANT MORTALITY
In the United States during 1934, according to the United States census reports, 2,167,636 infants were born alive. The birth rates per 1,000 estimated population in the expanding birth-registration area decreased from 25.1 in 1915 to 17.1 in 1934, or an average of about 2 percent per year. (See appendix table XI-1.) The census reports for 1934 also show that 12,859 women died from causes ascribed to pregnancy and childbirth; 130,185 infants died during their first year of life (73,841 of these dying during the first month) ; 43,175 children died at ages from 1 to 4 years, inclusive; 37,103 died at ages from 5 to 14 years, inclusive; and 26,885 died at ages from 15 to 19 years, inclusive. The social significance and waste of this loss of maternal, infant, and child life is evident. Deaths of infants under 1 year of age form 9 percent of the total deaths; those of infants under 1 month of age, 5 percent. The problem which confronts us--that of conserving the lives of infants and of women in childbirth--is, therefore, still very great. The magnitude of the problem is much greater if one considers as part of it the tremendous loss of fetal life. The registration of stillbirths is admittedly very incomplete, yet 78,503 stillbirths were reported during 1934. The causes of stillbirths and of the largest proportion of deaths of infants
261
during the first month of life are closely related to prenatal and natal conditions and to causal factors in maternal mortality. The prevention of death and disability associated with childbearing has therefore a significance which extends far beyond the preservation of maternal life and health for its own sake. It may be expected to decrease the losses of fetal and early infant life which form at the present time so large a proportion of infant mortality and further to lessen many child-welfare problems which are the direct results of homes broken by the loss of the mother.
Though there has been a downward trend in the maternal mortality rate in the United States from 1921 to 1934 (computed from the rates for the 26 States and the District of Columbia that have been constantly in the birth-registration area since 1921), the decrease has been slow, amounting on the average to only 1 percent annually, as the following figures for this area show
| Year | Maternal mortality rate | Year | Maternal mortality rate |
| 1921 | 67.3 |
1928 | 64.2 |
| 1922 | 65.4 |
1929 | 63.7 |
| 1923 | 65.8 |
1930 | 62.1 |
| 1924 | 64.0 |
1931 | 62.5 |
| 1925 | 64.3 |
1932 | 59.2 |
| 1926 | 64.6 |
1933 | 58.4 |
| 1927 | 62.3 |
1934 | 55.5 |
The rate of 59 for the whole United States in 1934{1} masks rates for different States ranging from 39 for Vermont to 87 for South Carolina. (See appendix table XI-2.) Figure 3 shows the number of deaths of mothers ascribed to causes related to childbirth per 10,000 live births in the several States. On this map the black areas represent the highest rates (75 or more). Only three States ( California, Vermont, and Wisconsin) are in the lowest group with rates of less than 45.
Differences are apparent when the rates are computed separately for white and Negro women and for urban and rural communities. In 1934 the rate for colored women in the United States was 90, as compared with 54 for white women. (See appendix table XI-3.) Though United States census reports in 1934 show the maternal mortality rate for urban communities to be 7l and that for rural regions only 50, studies in several States show that when deaths taking place in cities are reallocated to the place of residence of the women the rural rates are increased, often to a considerable degree, indicating that the rural problem is quite as important as the urban one. For instance, in New York State reallocation of deaths from 1927 to 1934
{1} The birth-registration area comprised all the States from 1933 on.
263
gives the following comparison with recorded rates available through 1931:
| Year | Urban {2} | Rural {3} | Year | Urban {2} | Rural {3} | ||||
| Recorded rate {4} | Resident rate {4} | Recorded rate {4} | Resident rate {4} | Recorded rate {4} | Resident rate {4} | Recorded rate {4} | Resident rate {4} | ||
| 1927 | 69.3 |
60.8 |
37.6 |
59.2 |
1931 | 67.1 |
57.5 |
37.2 |
57.1 |
| 1928 | 72.8 |
63.2 |
33.8 |
58.3 |
1932 | -- |
60.3 |
-- |
62.4 |
| 1929 | 68.5 |
61.0 |
31.9 |
51.0 |
1933 | -- |
60.3 |
-- |
55.1 |
| 1930 | 64.5 |
53.8 |
36.7 |
58.2 |
1934 | -- |
53.8 |
-- |
57.2 |
| {2} Places (exclusive of New York City) with population of 2,500 or more. {3} Places with population of less than 2,500. {4} Deaths per 10,000 live births and stillbirths. |
|||||||||
Figures from Ohio for 1930 and from Wisconsin for 1932 and 1933 show similar changes in rates as a result of reallocation to place of residence. Whether all deaths of rural women who die in urban areas are justly chargeable, to the rural area and whether all women who died away from home would have died if they had remained at home are questions that cannot be answered. The fact is, however, that distances to be traveled to obtain care and the frequent lack of regional hospitals and consultants make the rural problem of maternal care in many ways more difficult than the urban one. Recent, reports of studies of large numbers of individual maternal deaths have indicated the controllable nature of many of them, have brought out the inadequacy of care, and have pointed to the need for more widespread provision for prenatal and better obstetric care, including improved education of physicians, nurses, midwives, and the public as to what constitutes such care. Few women in rural areas or in the smaller cities have skilled nursing service at delivery. The need for the immediate provision of more adequate maternal care, including that given by physicians and by public-health or maternity nurses, and for education of both professional and lay groups is clear if lives of mothers in childbirth are to be saved. Because of the difficulties of making such provision in rural areas, attention should be especially focused on this aspect of the problem.
The United States has a poor record when its maternal mortality rate is compared with the rates for foreign countries. Appendix table XI-4 indicates the trend of maternal mortality in the United States from 1915 to 1934, together with similar data for certain other countries. The comparability of these rates has been challenged in the past on the basis that the procedure in ascribing deaths of women to causes connected with childbirth was not comparable as between the United States and different countries. An extensive study, in connection with the White House Conference on Child Health and Protection, has been made by the Children's Bureau in cooperation
265
with the Bureau of the Census, and the results of this study show that, in general, although there would be some changes if methods in use in certain foreign statistical offices were followed, the changes would be of minor importance. Unquestionably the United States has an exceedingly high rate as compared with the rates of most foreign countries.{5}
The map presented as figure 4, based on 1934 figures, indicates the great variation in infant mortality between the States. The solid-black States have rates of 75 or more infant deaths per 1,000 live births. In contrast with these are Oregon and Nebraska, which have rates of 40 and 45, respectively.
The reduction in infant-mortality rates as a whole since 1915 has been striking. (See appendix table XI-5.) In the group of States that have been constantly in the birth-registration area since 1921, this decrease has amounted on the average to 2.7 percent annually.
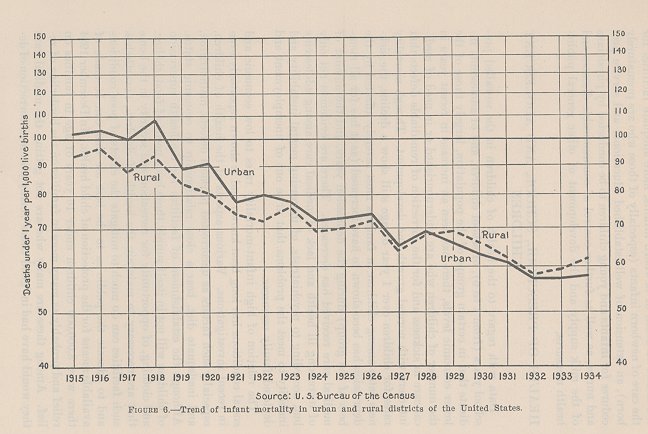
The reduction in total rates that has thus far taken place has occurred largely from the second to the twelfth month and can be accounted for to a great extent by education of the public in methods of infant care and by the effective operation of certain general public-health measures. The decrease in rates for infants dying under 1 month of age (neonatal death rate) has been relatively slow, amounting on the average to only 1.41 percent annually, while that for infants dying after the first month has averaged 4.14 percent. The decrease in rates for deaths due to prematurity has been even slower than that for all neonatal deaths, being 0.91 percent annually. Furthermore, the infant mortality rate of 60 in 1934 for the entire United States masks rates varying from 40 in the State of Oregon to 126 in New Mexico and rates of 55 among white infants and 94 among colored infants. (See appendix table XI-6.) In urban areas the decrease has been more rapid than in rural areas. Prior to 1929 the urban rate invariably exceeded the rural; since then the rural has been from 2 to 6 percent in excess of the urban. (See appendix table XI-7 and fig. 6.)
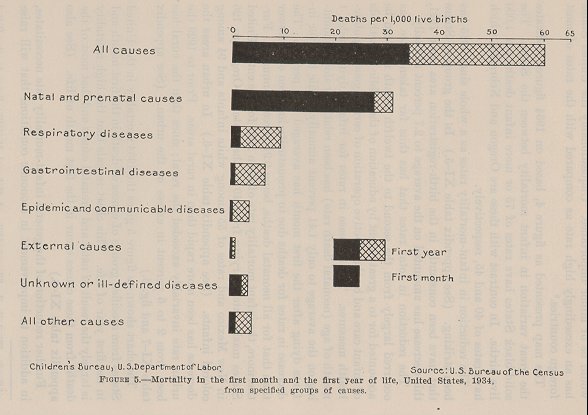
The chart shown as figure 5 gives the 1934 mortality in the United States from specified groups of causes of death in the first month and in the first year of life. This chart reveals that the high mortality is largely the result of natal and prenatal causes and that most of the deaths from these causes occur in the first month of life. (See also appendix table XI-8.)
Further reduction of the general infant-mortality rate necessitates, in addition to improvement in economic conditions that will raise
{5} Tandy, Elizabeth C., "Comparability of Maternal Mortality Rates in the United States and Certain Foreign Countries", U. S. Department of Labor, Children's Bureau Publication No. 29 (U. S. Government Printing Office, Washington, D.C., 1935).
267
standards of living, better maternal care, an increased knowledge of the causes of death of newborn infants, more adequate facilities for the care of newborn infants (especially of those who are prematurely born), an extension of well-established educational and service procedures for infants and young children to be conducted by physicians and nurses, as well as further control of communicable diseases and of the milk supply and the development of other general public-health measures.
HEALTH OF PRESCHOOL, SCHOOL, AND ADOLESCENT CHILDREN
Data with regard to the health of children in the so-called preschool years (from 1 to 6), of school children, and of adolescents indicate that in certain groups of the population, largely those of the lower economic levels, there has been an increase in recent years in the number of children who are undernourished or in need of medical care in sickness and for the correction of remediable defects that interfere with normal growth and development. Though mortality rates for children over 1 year of age still show a decline, the sickness rates among children in families most severely affected by the depression has been shown to have increased (as it has for all members of the group) during the depression years, and the amount of medical care received has decreased. There are evidences not only of increasing ill health and lack of medical care, among adolescents but, according to psychiatrists, of increasing mental instability and inability to meet the problems that arise out of unemployment and depleted family resources.
The relation of high infant-mortality rates to low economic and social conditions has long been known and is shown repeatedly even in recent investigations. Various aspects of the health of children, especially such factors as uncorrected physical defects, malnutrition, and inadequate diet, bear a close relationship to economic status. Although the establishment of facilities for the health supervision of children will not in itself supply those basic needs of food, shelter, and clothing, of opportunity for recreation and security in the home that are necessary to maintain the health of children, nevertheless such facilities can do much to mitigate the effects of poor conditions and to educate the public as to the best use that can be made of available means for the protection of child health. In December 1934 there were 8,000,000 children under 16 years of age in families on relief and probably as many more in families on the borderline of relief. Among these are many who are not getting the medical care they would have had in "good times", many who need correction of de-
269
fects, many who are not getting enough milk. The need for adequate health supervision for these groups of children is certainly greater than ever before.
DEVELOPMENT AND PRESENT STATUS OF PROVISIONS FOR
MATERNAL AND CHILD HEALTH
During the past 40 years there has been a gradual but steady development of the program for the protection of the health of infants and children and for better maternal care. Activities for the control of infant mortality, and subsequently for the prevention of maternal mortality, and the promotion of maternal and child health began in the large cities. The establishment in New York City in 1893 of the Straus Infant Milk Stations for the distribution of pasteurized milk for infant feeding is generally cited as the first large effort to control the diarrheal diseases of infancy. The establishment of similar infant milk stations by charitable organizations followed in other large cities. Although early efforts were directed and largely limited to providing pasteurized and "modified" milk for infant feeding, there gradually developed a realization of the necessity for preventing disease in infancy through providing opportunities for mothers to consult physicians regularly at these stations regarding the growth, physical condition, feeding, and general care of their children and to receive from the nurses attached to these centers home demonstrations in the care of the baby and the preparation of his food. As pasteurized and otherwise improved milk supplies became more generally available in cities, the work of the infant-feeding stations gradually became more educational in nature, and they became largely known as infant or child-health or welfare centers.
According to Dr. S. Josephine Baker,{6} by 1910 there were in the United States 42 organizations, located in 30 cities, maintaining some type of baby-health station. From 1921 to 1929, the period when the Federal Maternity and Infancy Act was in operation, 2,978 centers were established, chiefly in rural areas, for child-health, prenatal, or combined prenatal and child-health service. Some of these were discontinued after the act lapsed in 1929, but there are no figures to show how many ceased to operate. In 1930 a survey made by a committee of the White House Conference on Child Health and Protection showed that there were at that time, in addition to the consultation centers in rural areas, 1,511 permanent childhealth centers located largely in communities of more than 10,000 population. No exact information is available with regard to the number of child-health centers in 1934.
{6} Baker, S. Josephine, M. D., Child Hygiene (Harper and Brothers, New York, 1925), p. 215.
270
School health programs began in Boston in 1894 as a means for the control of communicable diseases. The first school nurses were employed in 1902 in New York City. In 1931, 4,422 nurses were giving full time to school nursing, and 3,376 were giving part time to this activity.
In 1908 the first bureau of child hygiene in a city department of health was established in New York City. Since then many municipal health departments have created such bureaus or divisions. The first division of child hygiene in a State department of health was established in Louisiana in 1912. From that year to 1917, seven more State divisions of child hygiene were set up, but during the years 1918, 1919, and 1920, when Nation-wide concern for the child was aroused as a result of the World War and the Children's Year campaign, 24 new State divisions or bureaus of child hygiene were organized. By the end of 1920, 32 States had established divisions or bureaus of child hygiene. In 1921, the year of the passage of the Maternity and Infancy Act, 4 States created divisions of child hygiene and in 1922 and 1923, 11 more did the same. Thus, by the end of 1923 all the States except one had such a division. In 1925 Hawaii reported the formation of one.
It was not until 1912, with the establishment of the Federal Children's Bureau, that special Federal activities on behalf of child and maternal health were begun. Previous to this time the only Federal activity relating especially to this matter was that of the United States Public Health Service in connection with its studies of the relation of contaminated milk to infant mortality, reported in 1909.
The need for more widespread maternal and child-health measures was revealed by Children's Bureau studies of social and economic factors in (1) infant mortality, (2) conditions of maternal, infant, and child welfare and health in rural areas, and (3) maternal mortality. Added weight was given by the discovery of such large numbers of physical defects in men examined during the World War under the draft, many of which defects, it was thought, could have been prevented had proper health care been given during childhood; the Children's Year activities in 1918, during which some 7,000,000 preschool children were weighed and measured and, where possible, given medical examinations, which showed many children to be suffering from preventable and remediable defects; the demonstrations in New York and Boston and other communities of the benefits of prenatal care to maternal and infant health; the continued demonstrations in urban communities of the beneficial effect of infant health supervision on the death rate of the infants who received such supervision; and the results of many other observations and investigations. All
271
this evidence led ultimately to the demand for national effort for the protection of the health of mothers and children, and resulted in the passage by Congress in 1921 of the so-called Maternity and Infancy Act for Federal-State cooperation in the promotion of the welfare and hygiene of maternity and infancy. This measure was in operation for 7 years, from 1922 to 1929.
The work done by the cooperating States and by the Federal Government under this act is reviewed in detail in the annual reports of the administration of the act. In the program were included the establishment of permanent and itinerant prenatal, infant, and preschool-child health centers and conferences in counties and local commuities through the divisions of child hygiene of the State departments of health, the placing of nurses in counties to develop county-wide programs of maternal and child health, and the development of many types of educational programs for mothers and other lay groups. In some States special demonstration programs were carried out by the Division of Child Hygiene in cooperation with medical, nursing, and other local groups. The study of more than 7,000 maternal deaths in 15 States was one of the most important research activities of this program.
To evaluate the results of the child-health program as it has developed and expanded throughout the years and to distinguish them from the effects of changing economic conditions is not possible on a large scale. The results of a long educational and service program are cumulative and the effects of good times and improved health services carry over into periods of depression and less adequate service. That infant-mortality rates did not begin to go up until 1934 may be attributed in no small degree to the earlier education of mothers and various lay groups in infant and child health. But credit must be given also to the relief measures more recently instituted by local, State, and Federal agencies throughout the Nation, which in a number of States have included increased public-health nursing and child-health activities developed as part of the program for emergency relief. As has been pointed out, there is unquestionably definite evidence at hand from demonstrations in individual communities that educational and service programs have a definitely beneficial effect on child health--an effect such as to justify fully an expansion of the maternal and child-health program in all States.{7} But State funds for such expansion are not available in most States, and many States are more seriously handicapped in their programs today than for a number of years past because of
{7} The need for expansion is emphasized by the fact that the infant-mortality rate for 1934 was significantly higher than that for 1933.
272
reduction in the appropriations to State health departments for maternal and child health. (See table 57.)
By 1927 all the States except three were receiving Federal funds under the terms of the Maternity and Infancy Act. During 1928 the States had apprdximately $2,158,000 for maternity and infancy work, of which about $1,140,000 was from State funds. Following the expiration of the act, the legislatures in a number of States increased their appropriations for maternal and child health, in some instances in an amount that exceeded the previous combined Federal and State funds.
273
However, in 1934 funds for this work reported to the Children's Bureau by the State departments of health had been reduced to approximately $1,157,000 and nine States reported no special appropriations for this purpose. Of the 39 States and Hawaii which reported funds for maternal and child-health work, 5 reported increases over amounts expended in 1928 and 35 reported decreases, the latter ranging from 0.9 percent in Rhode Island to 96.1 percent in Alabama. It is significant that 22 of these States and Hawaii reported funds in 1934 which were less than 50 percent of those expended in 1928.
To recapitulate, at the expiration of the Maternity and Infancy Act in 1929, or soon thereafter, appropriations equaling, nearly equaling, or exceeding combined Federal and State funds had been made by the legislatures of 21 States and Hawaii, but in 1934, 17 of these 21 States and Hawaii reported "no special appropriation" or reported decreases in funds for maternal and child-health work as compared with 1928.
Consideration of relative degrees of curtailment of funds does not bring out the grave inadequacies in some States which are disclosed by analysis of the actual amount available for maternal and childhealth work in 1934. This inadequacy is strikingly illustrated in table 58, which shows that State funds for expansion of the maternal and child-health program are not available in most States. This table
274
shows that 23 States and Hawaii had less than $10,000 for maternal and child-health work for 1934, and of these, 14 had no special funds for maternal and child health or less than $3,000; 14 States had between $10,000 and $30,000; 6, between $30,000 and $50,000; and only 5, more than $50,000.
Other evidence of the lack of resources in many of the States for effective maternal and child-health activities, particularly in rural areas, is seen in the general inadequacy of such accepted measures as public-health nursing service in counties and permanent prenatal and child-health centers conducted by physicians. One of the most effective ways of reaching the problem of infant and maternal mortality and health protection of children is the development of public-health nursing services, because it is through these services that the mothers are made to realize what kind of medical attention is needed and how important it is to place themselves under the care of a physician early in pregnancy; also it is through the public-health nurse that the mother learns how to take care of the baby and to give the child the best possible start in life.
The extent to which the mothers and babies of this country are without the essential services has been shown by certain studies. For example, the public-health nurse is a valuable agent in decreasing maternal and infant mortality. Her services include advice to the mother during pregnancy and instruction in feeding and caring for the baby, of course under medical instruction. Reports have been made of the public-health nursing services available in 1934 in the counties of 24 States which average fairly well in the provision for public-health service. ( See table 59. ) Of 1,018 rural counties in these States, only 364, or about one-third, including 46 percent of the population, had any permanent county-wide nursing service in 1934. Thus 54 percent of the population in these counties was without any service of this kind. Frequently in a county having county-wide nursing service one nurse serves the entire county.
Another very important aspect of the maternal and child-health program is the provision of health centers where mothers can go for advice, consultation, and examination, both in the prenatal period and with the children after the children are born. This service is developed in close relation to the public-health nursing services. Figures are available on the number of prenatal and child-health centers in the counties of 18 States in 1934, and here, again, these 18 States do not represent the most needy group. They represent States from which information could easily be obtained. In the urban counties of
275
those States 55 percent had prenatal or child-health centers, but in the rural counties only,11 percent had such centers. Table 60 gives the figures on which these statements are based.
| TABLE 59.- Permanent public-health nursing services in the counties of States, 1934 {1} | |||
Types of nursing services |
Number of |
Population of counties {2} |
|
Number |
Percent |
||
| Total counties in states | 1,393 |
76,887,743 |
100 |
| Permanent nursing service | 834 |
68,074,901 |
89 |
| County-wide service | 629 |
51,354,807 |
67 |
| Local service only | 205 |
16,720,094 |
22 |
| No permanent nursing service | 559 |
8,814,842 |
11 |
| Total rural counties in states | 1,018 |
19,754,839 |
100 |
| Permanent county-wide nursing service | 364 |
9,042,631 |
46 |
| No permanent county-wide nursing service | 654 |
10,712,208 |
54 |
| {1} Compiled from data received by U.S. Children's Bureau from State health departments. {2} U.S. Department of Commerce, Bureau of the Census, Fifteenth Census of the United States: 1930, "Population (U.S. Government Printing Office, Washingon, D. C., 1933). |
|||
| TABLE 60. Permanent prenatal and child-health centers in the counties of 18 States, 1934 {1} | ||
Prenatal and child-health centers |
Number of |
Percent |
| Total counties | 982 | 100 |
| Prenatal and child-health centers | 220 | 22 |
| Both prenatal and child-health centers | 137 | -- |
| Prenatal centers only | 6 | -- |
| Child-health centers only | 77 | -- |
| Neither prenatal nor child-health centers | 762 | -- |
| Urban counties | 261 | 100 |
| Prenatal and child-health centers | 144 | 55 |
| Both prenatal and child-health centers | 97 | -- |
| Prenatal centers only | 4 | -- |
| Child-health centers only | 43 | -- |
| Neither prenatal nor child-health centers | 117 | 45 |
| Rural counties | 721 | 100 |
| Prenatal and child-health centers | 76 | 11 |
| Both prenatal and child-health centers | 40 | -- |
| Prenatal centers only | 2 | -- |
| Child-health centers only | 34 | -- |
| Neither prenatal nor child-health centers | 645 | 89 |
| {1}Compiled from data received by U.S. Children's Bureau from State health departments. | ||
276
Such reports indicate very clearly that large groups of the rural population were at that time without any public-health nursing or permanent prenatal and child-health conference service. How much prenatal or child-health service was given by private physicians in these regions is not known.
Evidence is also available of a striking dearth of a service which is a recognized necessity for adequate maternity care, namely, the provision of home-nursing service at delivery and postpartum for patients who cannot pay for such nursing care. Reports on this subject were received by the Children's Bureau in 1934 from 27 States. Of these 27 States, 9 reported no provision whatsoever for a permanent maternal home-nursing service. Eight States reported permanent maternal nursing services in some towns of less than 10,000 population and 12 States in some cities of more than 10,000 population. No State reported a rural county-wide maternal nursing service.
Although in cities and towns maternal and child-health services are more often available than in rural areas, in many urban communities there have been decreases in appropriations or in funds raised through private sources. Such reductions in funds, as well as the increasing load of bedside nursing service required, have curtailed to a considerable extent activities of public-health nurses in the field of maternal and child health, and even in some of the largest cities child-health conferences have been reduced. In rural areas and in communities of small population, organized facilities for these services to mothers and children had always been far from adequate, even when Federal funds were available to assist States in this program, and later they became still more inadequate, as has been shown, because of curtailment in the resources of the State health departments, local boards of health and education, and private agencies.
The need for State leadership, particularly in rural areas, in the development of local child-health work, as well as in the general health program, is well recognized. With the limited funds available in 1934 for maternal and child health, such leadership was impossible in a large number of the States.
The need for public-health nursing service and medical care for children was shown by reports made in 1934 of visiting nurses in 25 cities, relating to 9,472 children in 3,500 families, shown in table 61. The number of children reported as having defects that needed attention was 31 percent of the total number. These reports were not based on medical examinations, which would have revealed a great many defects not obvious to the mothers and the nurses. Treatment was not arranged for in almost half of the cases reported as having defects. In 833 of the approximately 1,300 cases in which treatment was not arranged for, the reason given was financial distress.
277
Table 62, based on this same group, shows the adequacy of milk supply in these families. In the total group 56 percent of the families were receiving less than 50 percent of the milk estimated to be necessary on the basis given in the table. These families were divided into those receiving relief and those not receiving relief. Sixty-four per cent of the families receiving relief had a milk supply less than 50 percent adequate, as compared with 49 percent of the families not receiving relief.
PLAN FOR EXPANSION OF MATERNAL AND CHILD HEALTH PROGRAM
In view of the facts and conditions outlined, it is believed that a program should be developed, especially in rural areas and in areas in special economic need, that will permit the Federal Government through the Children's Bureau to cooperate with the States and Territories in the promotion of the health and welfare of children and mothers. The general program would be one of consultation, education, and demonstration services, with aid to States and Territories, and through them to local communities, and would involve State and local administrative leadership by public-health authorities in close cooperation with medical groups. It would also be assumed that such a program for the promotion of maternal and child health would require cooperation in planning and in procedure with Federal and State authorities that are administering other, phases of the, public-health program, with those departments of Federal and State gov-
278
ernments that have to do with administration in the fields of social welfare, education, and labor, and with other national and State professional and lay organizations. In addition to the general program for maternal and child health, special programs are suggested for demonstration and research in the development of more adequate provisions for maternal care of women in rural areas and for the care of crippled children in the smaller cities and towns and rural areas.
In the furtherance of the general program of maternal and child health, special consideration should be given (a) to local services for children and mothers-services to be administered by local public-health units with the use of combined local, State, and Federal funds; (b) to conditions in rural and other especially needy areas; (c) to the development of demonstration services or services of a more permanent character in localities in special need; and (d) to the development of adequate divisions of maternal and child health in State departments of health that can provide the leadership and administrative assistance necessary to develop local services and State-wide
279
maternal and child-health educational activities. In such a program, though the lives and health of mothers, infants, and young children may be considered as a major responsibility, attention must also be given to the physical and mental health needs of children of all ages, especially to those problems that have to do with mental health and its relation to delinquency, with the health of adolescents in school and of youths who are seeking employment or are already in industry, with the health needs of special groups of children, such as children who are physically or mentally handicapped, children in institutions or foster homes, children in families in which the father is dead or absent from home because of illness or desertion, and children in families on relief rolls.
LOCAL PROGRAMS FOR MATERNAL AND CHILD HEALTH
In planning a local health program for mothers and children in counties or districts, especially in rural areas and small centers of population, it is believed that emphasis should be placed on the development by the health authorities, in cooperation with medical and other local groups, of certain minimum health services for mothers and children unable to obtain them otherwise, and, on State and local programs for education of lay and professional groups in the essentials of adequate maternal and child care. The use of local committees on child health and welfare (composed of representatives of local professional and lay groups) to assist in developing the educational program, in establishing the minimum services; and in extending them to meet local needs should be considered in developing any plan. Such health services for counties and local communities with special reference to rural areas may include the services outlined in the paragraphs which follow.
Local Medical, Dental, and Nursing Service.-These services are to be provided preferably by local physicians and dentists qualified to do the special work required and by full-time public-health nurses employed by health departments, working under the general supervision of the health officer and other physicians. The physicians and dentists should be paid by the local health department for their services. When local practitioners are not available, other arrangements for the various services may be made. The educational and preventive aspects of both maternal and child-health services should form an important part of the service rendered by physicians and dentists. In all the health services full cooperation of local medical and dental groups should be obtained.
The medical, dental, and nursing service program should consist of the following five major categories:
280
(1) Prenatal, infant, and preschool services:
(a) In permanent conferences located in the center or centers of population of the county or district.
(b) In regular itinerant conferences reaching out from such centers to rural areas of the county or district.
(c) In physicians' or dentists' offices when found to be practicable and advisable by health and medical groups.
(2) School health services, including health examinations and health-education programs, to be provided preferably by local physicians through the local departments of health or education, or both, in a cooperative program with medical groups in the community.
(a) Health examinations (including dental) of all children on entering school and at stated intervals thereafter and of other children as indicated. Special attention should be given to highschool children and to children leaving school for work, and emphasis should be placed on the part played by health examinations in the health-education program.
(b) Follow-up. Plans should be formulated by physicians with nurses, social workers, nutritionists, and others for adequate follow-up for correction of defects.
(3) Health service to children entering employment or at work. An educational and health-service program, including medical and dental examinations, carried out by health agencies in cooperation with school authorities, junior employment agencies, or other social services existing in the county, district, or other local community.
(4) Health service to special groups of children, such as handicapped children, children in institutions, and children in families on relief, carried out in cooperation with social-welfare agencies of the county, district, or other local community.
(5) Public-health nursing service for mothers and children.
(a) As part of the generalized service of the official county or district health units, primarily an educational and demonstration program.
(i) Home visiting in connection with the maternal and child-health program in all its phases.
(ii) Service at prenatal and child-health conferences.
( iii ) Assisting at school health examinations and in conference with parents and teachers for the purpose of securing correction of remediable defects.
(iv) Cooperation with physicians, county welfare and education authorities, nutrition and extension workers, and lay organizations in connection with health supervision of individuals and in bringing about community organization for improved health services for all mothers and children.
(b) Maternity. Nursing service for care of mothers at delivery and postpartum; a bedside nursing service and educational program in maternal care for the women of the county and local communities. ( Such service as this is provided now as part of the generalized program or as a specialized program in a number of cities. It has been developed but little in small towns and cities and, with the exception of a few demonstrations, not at all in rural areas.)
281
Provision for Medical Care in Connection With Maternal and Child-Health Program.-Though it is not the function of physicians conducting a health service to render general medical care to the sick, it should be their responsibility as part of a preventive program and in cooperation with local medical, nursing, welfare, and social-service groups to see that provision for adequate care is made through private physicians and dentists or, in the case of children in families unable to provide the necessary care, through appropriate welfare agencies. In the maternal and child-health field this is especially necessary for the correction of remediable defects that handicap the normal growth and development of children and for the provision of adequate obstetric care of women at and following delivery. Plans for cooperation with hospitals, convalescent homes, and other institutions for care of the sick or handicapped should be worked out with medical social workers and others.
Educational Program.-A continuing program of education in the essentials of adequate maternal and child care should be developed by local county or community health services in cooperation with medical groups, educational authorities, nutrition experts, and others. Though such a program of education is probably carried out most effectively in the form of the individual instruction of health officials, physicians, and nurses already outlined, it should also include (a) health instruction in schools, (b) group instruction of adults, (c) community organization for the establishment or improvement of health services for mothers and children, and (d) the use and distribution of printed matter, such as bulletins and posters on child and maternal health, emphasizing preventive measures, health habits, nutrition, and general standards of good care. Education in the field of mental health may be developed through any of these channels as qualified personnel becomes available for this aspect of the total health program.
STATE-WIDE PROGRAM
In order to develop local health services for the promotion of the health of mothers and children, leadership must come from the State health department through its division of maternal and child health and, for those local communities unable to develop even minimum services, assistance is also necessary in the form of funds or personnel, or both. The function of a division of maternal and child health is primarily advisory and educational in nature, the program developing along the lines of (a) consultation with and guidance of local communities in developing their services for mothers and children, (b) demonstration of services in local communities for which personnel may need to be provided, (c) assistance in the provision of more
282
permanent services in localities in special need, and (d) State-wide educational programs for promotion of maternal and child health. In its activities the division should work in close cooperation with other divisions of the State health department, all of which have functions that are fundamental to the health of mothers and children. In the same way cooperation by the division with State departments of welfare, education, labor, et cetera, is essential to a comprehensive program of child and maternal health. Furthermore, because many of its services are primarily clinical in nature, the division must work closely with those medical groups that are specially concerned with the health of children and mothers and also with the general medical groups of the State and local communities.
To fulfill its function a division of maternal and child health might well have a staff as follows:
A director who should be a physician, preferably one trained in the clinical aspects of pediatrics or obstetrics and with experience in child and maternal-health activities.
(a) Additional medical state for consultation and advisory service composed of full-time or part-time physicians with training and experience in either child or maternal health, the size of such state to depend on the needs of individual States. To this medical state a full-time dentist should be added.
( b ) Part-time regional consultants in the fields of pediatrics, obstetrics, and dentistry.
( c) State supervisory and regional advisory nurses, trained and experienced in public-health nursing, preferably with special experience in maternal and child-health activities.
(i) Part-time service of field nurses carrying a generalized public-health nursing program for the purpose of demonstration in cooperation with other divisions of the health department in counties where needed to promote interest or to supplement budgets temporarily.
(ii) Field nurses for special demonstration programs.
(d) Additional special staff in fields of nutrition, mental hygiene, health education, etc.
The activities of the State division of maternal and child health might well be divided into those which are administrative, those which have to do with health services or special demonstrations to be developed on a State-wide or local basis, and those which are largely educational in nature. The organization of State-wide or local health services or educational programs should be carried out in cooperation with other divisions of the State health department and with local health and medical groups. Where State and Federal funds are available for local purposes the State division would probably assist in formulating plans and should have the responsibility for approving them. The activities of the division should be flexible, so that
283
new programs may be developed from time to time and new methods of administration or demonstration tried.
The development, in collaboration with local health units, of an educational program that would reach all groups, both lay and professional, would be an important responsibility of the State division. Such an educational program might include:
(1) The development of State-wide planning, in cooperation with medical and other professional groups, for education of parents and lay groups in the essentials of adequate maternal and child care, with special emphasis on the ways and means of obtaining these essentials through local physicians, health departments, etc.
(2) Cooperation with professional groups (medical, nursing, social welfare, education, home economics, etc.) in the development of a continuing program of education of these professional groups in the form of institutes, refresher courses, etc., that will bring to physicians, nurses, and others current knowledge in the fields of pediatrics and obstetrics and their practical application in the county-wide program of child and maternal health.
(3) The continued instruction of midwives and subsequent raising of standards of licensing that are an important part of this program of education.
(4) Cooperation with departments of public instruction and other education groups in developing an educational program for students in high schools and vocational schools, in normal schools, and in colleges in the essentials of maternal and child care.
CARE FOR CRIPPLED CHILDREN
Another large group of children for whose needs, from the point of view of diagnostic services, medical treatment, and convalescent care, very inadequate and uneven provision is being made are the crippled and those suffering from chronic diseases, such as heart disease and tuberculosis. The actual number of such children is not definitely known, and many of the general estimates of need are based on surveys in urban areas, but State-wide surveys to discover crippled children have given definite evidence that a large number of children in rural and small-town areas will be forced to go through life with severe handicaps unless more public funds are made available for their care.
By 1934 some provision had been made in 37 States for a State department or commission or a State hospital to undertake special services for crippled children, and 35 of these States {8} (table 63 ) have made appropriations for this purpose. Except in a few States in which funds are available only for hospital care, the services pro-
{8} The statutes of North Dakota and Wyoming authorize a State department to provide care for crippled children, but no special appropriations have been made for this purpose.
284
vided include the location and registration of crippled children by surveys or by a school census; development and extension of diagnostic and follow-up clinics--either permanent or itinerant or both--staffed by a physician and a nurse and assisted by county social workers and physiotherapists; and the provision of medical and nursing care and after-care, in the child's home, in a hospital, in a convalescent home, or in a foster home.
In the different States the agencies charged with responsibility for locating crippled children and seeing that needed care is given vary greatly. In some States this work is done by a special commission for crippled children; in others by the department of health, public welfare, or education; in others it is a cooperative service of two or more of these departments. The basis for this variation lies in the combined medical, social, and educational services that are needed by the crippled child, often during a period of years, to assist him in overcoming his handicaps. The most effective agency is the one that can best coordinate the resources of the State for this work.
It is estimated that approximately $5,500,000 is spent annually from State and county funds for the care of crippled children. As is shown in table 63, State funds have been appropriated for (1) a general program of care, including clinics, treatment, and rehabilitation, and (2) for hospital service, either in special orthopedic hospitals or in general hospitals, usually State university hospitals, which provide a special orthopedic service. A large part of all appropriations is spent for hospital care, since as a rule surgical and medical care must be provided out of the appropriations for the general program. In addition to State funds, county funds are reported for 11 States, the largest county expenditures being made in New York and Ohio. In New York the counties reimburse the State for half its expenditures for this purpose, in Ohio for the entire sum.
In addition to State and county funds, it is probable that a fairly large sum is spent annually by municipalities for orthopedic care, although no data are available on this point. In the cities are also found the strongest of the private organizations for crippled children and the bulk of private funds for their care. It is difficult to judge from the reports of services provided by State agencies the extent to which State services are provided for children in the large cities. An analysis of the number of children under care in four States (New York, Ohio, West Virginia, and Wisconsin) showed that from 59 to 100 percent of the children were from counties that did not include a city of 100,000 or more population.
285
286
The amounts of public funds that have been made available in the different States vary widely, and in many there is great need for more adequate public provision for saving children from serious crippling conditions. Reports indicate that services formerly available have been curtailed during the depression and that in many instances needed care has not been given because of financial distress of the family or the community. On the basis of the experience of States having the most comprehensive programs, it is estimated that between 8 and 9 million dollars of combined Federal, State, and local funds are needed for these children at the present time. The need for services in any State may be greatly increased by an epidemic of poliomyelitis or infantile paralysis, which has been shown by various studies to have been the cause of crippling from 15 to 51 percent of the children needing care. It is most important, therefore, that Federal funds be so distributed that these special needs will be met.
The types of services that have been outlined are largely restorative, preventive, and general medical and health services. There is need also for the development of educational opportunities for crippled children, especially in rural areas, and State programs for physical restoration must be closely allied with State educational programs, especially the program for vocational rehabilitation of handicapped children 14 years of age or older.